HV Stent Plus
You are here:
- Home
- GASTROENTEROLOGY
- Esophageal stents
- HV Stent Plus
Are you interested
in this
product?
HV Stent Plus
Personal references
Prof. Hans-Ulrich Laasch, Dr. med. MRCP FRCR
The Christie NHS Foundation Trust, Manchester, UK
“The HV+ stent has shown itself to have one of the lowest migration rates across the gastro-oesophageal junction and could be demonstrated to stay in position where other stents have displaced."
As a braided, fully silicone encapsulated stent, it has a relatively high axial rigidity, which may cause issues in tight anatomical flexures, but the related high expansion force make it particularly suitable for bulky tumours."
"Due to the markedly increased survival of patients after oesophageal stenting, stent durability and removability have become a much more essential property than was previously necessary. Perishing of stent coverings and failure of the stent skeleton through nitinol corrosion is now frequently observed in our institution. The HV+ is one of the most corrosion resistant stents on the market, usually allowing definitive palliation. "
"Where revision is required, it can be reliably removed, even after many months in situ. The steel retrieval wire is easy to identify and capture, allowing extraction of the stent, thus increasing the options for re-intervention without limitation by an existing stent.”
As a braided, fully silicone encapsulated stent, it has a relatively high axial rigidity, which may cause issues in tight anatomical flexures, but the related high expansion force make it particularly suitable for bulky tumours."
"Due to the markedly increased survival of patients after oesophageal stenting, stent durability and removability have become a much more essential property than was previously necessary. Perishing of stent coverings and failure of the stent skeleton through nitinol corrosion is now frequently observed in our institution. The HV+ is one of the most corrosion resistant stents on the market, usually allowing definitive palliation. "
"Where revision is required, it can be reliably removed, even after many months in situ. The steel retrieval wire is easy to identify and capture, allowing extraction of the stent, thus increasing the options for re-intervention without limitation by an existing stent.”
Natalia V. Lozhkina MD, PhD, Head of endoscopic department of the State Autonomous Healthcare
Institution of the Perm region, Clinical Hospital №4 of the Perm city
‘’The main criterion of my choice is ergonomics. HV Stent Plus meets all requirements for a convenient and predictable implantation and is also characterized by safe removal from the esophagus with minimal risk of bleeding. Stents of this design are comfortable for the patient compared to other models. They have minimal complications compared to other models in dynamic 1-2 year follow-up observation’’.
Sergei V. Zhuravlev, MD
Head of endoscopic department of the Irkutsk Regional Cancer Centre
‘’Since 2004 I have been using HV Stent Plus in my daily practice and have performed more than 1000 implantation. My choice was based on the unique antimigration design that allow to get the minimal distal migration rate in the low part of esophagus and makes me in the quality of conducted treatment’’.
Natalia V. Tchueva, MD
Head of diagnostic department of the Belgorod Regional Cancer Centre
“For me as a specialist it is very important to be sure in quality of conducted therapy. HV Stent Plus has CE mark and extensive scientific evidence-based data. All of this allow me to get perfect clinical outcomes and get positive feedback from my patients.”
Basic description
The HV Stent Plus is a fully covered self-expandable esophageal stent with a unique anti-migration design that combines the benefits of partially covered and fully covered esophageal stents. The low migration rate and prevention of tissue ingrowth is complemented by safe and reliable extractability. If the stent is implanted in the distal part of the esophagus and protrudes into the cardia, it may be equipped with an anti-reflux valve that prevents reflux of gastric juices.
Indication
The HV Stent Plus is intended for patients aged 18 and older and indicated for palliative treatment of malignant dysphagia, for sealing malignant esophagorespiratory or esophagomediastinal fistula. The device can be temporarily implanted in patients with refractory benign esophageal strictures.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Features / Benefits
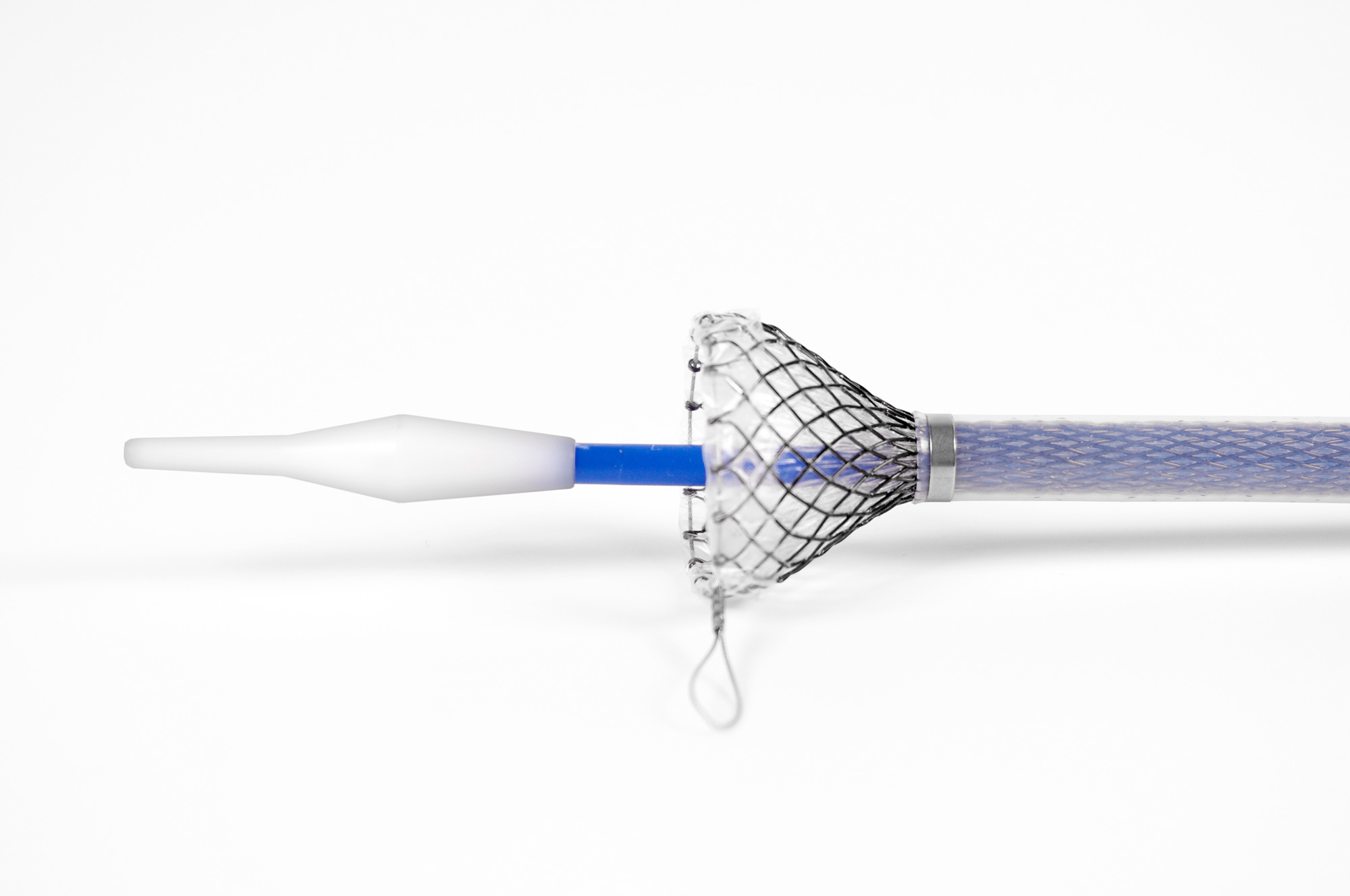
The stent has a minimal migration rate due to its anti-migration design, which is secured by a unique collar at the proximal stent end.
There are metallic retrieval loops with high strength and resistance to acidic environment at both stent ends.
The retrieval loops in combination with centripetally tapering flares allow safe and ergonomic removal of the stent from the esophagus.
The stent has a high radial force for effective dilation of the stricture and resistance to external pressure.
The HV Stent Plus is fully covered by durable silicone, which prevents tumor ingrowth into the stent and allows easy extraction. At the same time, the covering protects the nitinol mesh from contact with stomach acids and potential corrosion.
Platinum-iridium markers located at both ends, in the middle of the stent and on the anti-migration collar ensure visibility of the stent under X-ray.
The stent has atraumatic fully covered flares that reduce esophageal wall irritation and tissue response.
The universal low-profile and flexible 16/22 F delivery system allows easy insertion even into tough stenoses.
If the HV Stent Plus is implanted in the distal part of the esophagus, it can be equipped with an anti-reflux valve.
MRI compatibility – “MR Conditional”, compatible with 1.5 Tesla and 3 Tesla static magnetic field.
Patent protected
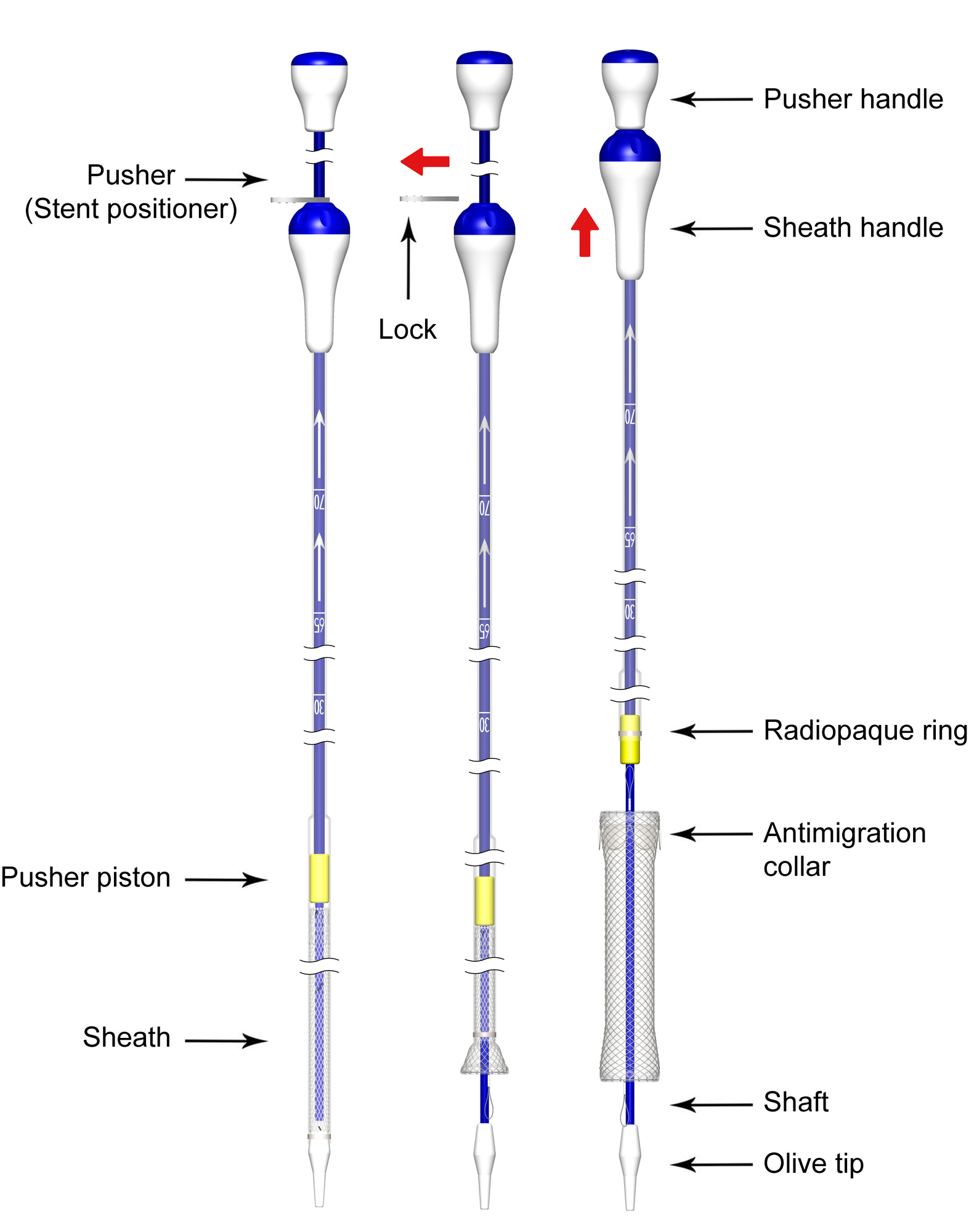
Implantation
The stent is delivered sterile and compressed in the delivery system. We recommend using a 0.035 ”(0.89 mm) / 220 cm ultra-stiff guidewire for the implantation.
Available sizes
| REF No. | Stent diameter [mm] Proximal flare / Body / Distal flare | Stent nominal length [mm] | Anti-reflux Valve | Delivery system |
|---|---|---|---|---|
| 019-09SL-20-085 | 25 / 20 / 25 | 85 | No | 16 F / 22 F |
| 019-09SL-20-110 | 110 | |||
| 019-09SL-20-135 | 135 | |||
| 019-09SL-20-150 | 150 | |||
| 019-09SL-20-085-O | 85 | Yes | ||
| 019-09SL-20-110-O | 110 | |||
| 019-09SL-20-135-O | 135 | |||
| 019-09SL-20-150-O | 150 | |||
| 019-09S-18-085 | 25 / 18 / 25 | 85 | No | |
| 019-09S-18-110 | 110 | |||
| 019-09S-18-135 | 135 | |||
| 019-09S-18-150 | 150 | |||
| 019-09S-18-085-O | 85 | Yes | ||
| 019-09S-18-110-O | 110 | |||
| 019-09S-18-135-O | 135 | |||
| 019-09S-18-150-O | 150 |
Publications
ELLA-HV anti-migration stent demonstrates superior performance for cancers of the gastrooesophageal junction
Mercer J, Najran P, Edwards DW, Borg P, Mullan D, Bell J, Laasch H-U
BSIR Annual meeting, Birmingham, 1st to 3rd Nov 2017
Oesophageal stents with anti-migration design: Getting a grip on stent displacement
Philbin CA, Stivaros SM, Mullan D et al.
BSIR Annual meeting, Manchester, 13th to 15th Nov 2013
A comparison of oesophageal self-expanding metal stents and their complications
C. Davidson, C. Rutherford, J. Allan, G. Simpson, J. Gray. (2016)
Royal Alexandra Hospital, GGC NHS Trust, Glasgow, UK.
International Journal of Surgery. 36. S88. 10.1016/j.ijsu.2016.08.294.
Fully covered stents versus partially covered stents for palliative treatment of esophageal cancer: Is there a difference?
J.O. Alonso Lárraga, D.Y. Flores Carmona, A. Hernández Guerrero, M.E. Ramírez Solís, J.G. de la Mora Levy y J.C. Sánchez del Monte
Departamento de Endoscopia Gastrointestinal, Instituto Nacional de Cancerología, Ciudad de México, México Recibido el
30 de septiembre de 2016; aceptado el 5 de julio de 2017
For more information on publications, visit our Education section.