Education
Here you will find information for patients as well as for healthcare professionals.
for patients
Stent
A stent is a mesh tube that works as a reinforcement to restore the patency of a narrowed anatomical tube (digestive tract, airways, etc.) caused by a benign or malignant disease or tissue injury.
The stent is usually made of nitinol (nickel and titanium alloy, coated with a special coating), which is characterized by shape memory, elasticity and a corresponding radial force. It is a safe, standard and established method.
The stent is implanted for a fixed period followed by its extraction or as a permanent solution.
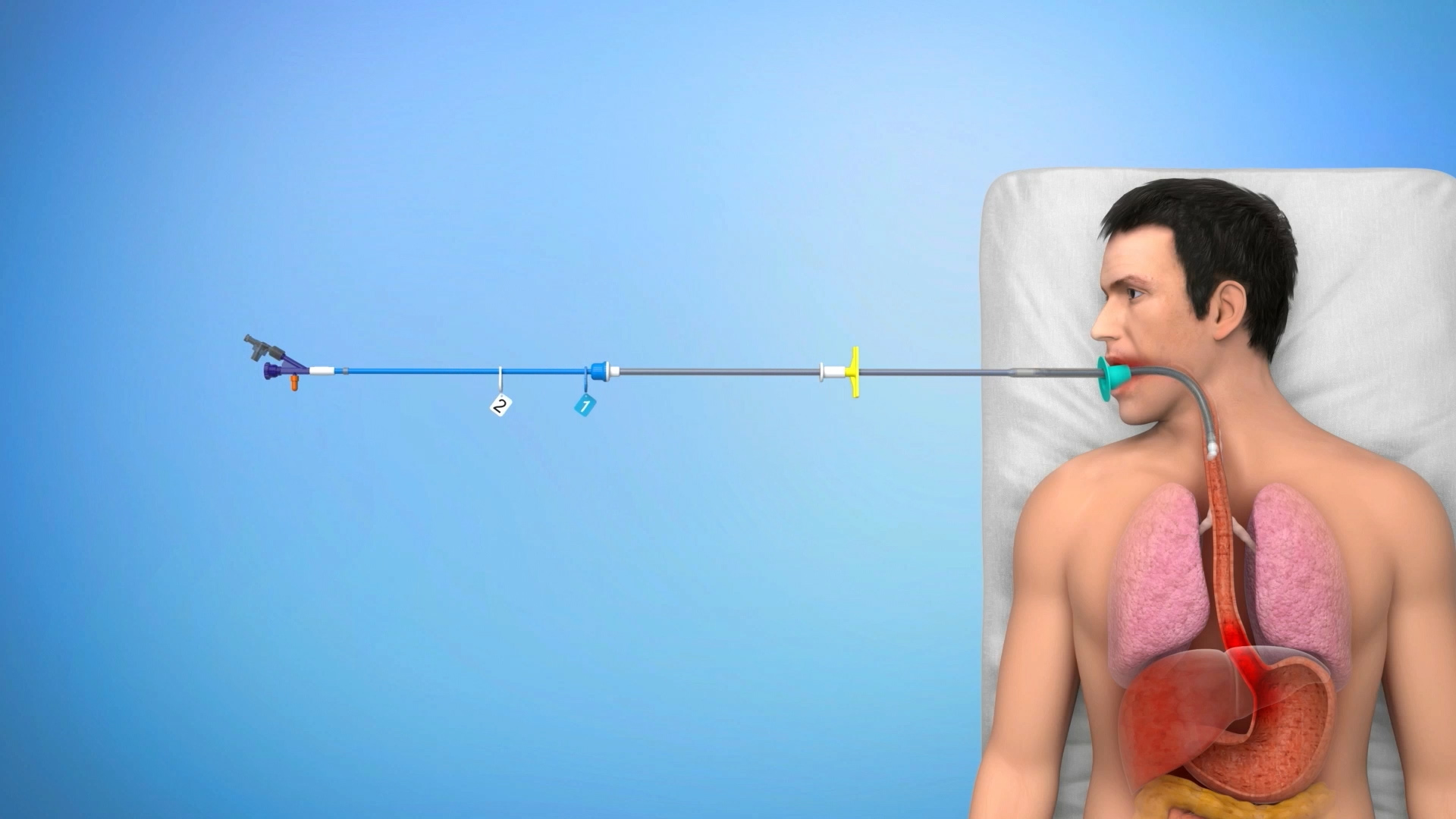
How is the stent implanted?
All our stents are self-expandable (they open themselves) and are inserted through natural body orifices, or, in the case of specific stents intended for biliary ways, they can be inserted through the side of the body through a catheter.
Gastrointestinal stenting is associated with a high degree of safety and technical success.
Before stent implantation
Examination before the procedure (recommended and arranged by the attending physician):
Coagulation control – hemocoagulation values of blood. Allergic history, common colds, infectious or other immune diseases. Previous radio-chemotherapy. Overall condition of the patient. Pregnancy.
Instructions for the patient before the procedure:
Interruption of food intake (fasting) at least 4 to 6 hours before the procedure in the esophagus (fluid intake is allowed). In case of implantation in the large intestine, avoid the solid food the whole day, drink only clear liquids, in addition, omit foods with a large amount of indigestible residues 5 days before the examination.
After stent implantation
In the case of a visit to another specialist (different specialization), please inform him in advance about the inserted metallic stent (this applies especially to X-ray, CT, NMR, ultrasound examinations).
After implantation of an esophageal stent, there is a common feeling of chest tightness or mild pain, which should disappear within approx. 1 week. In case of any problems, persistent pain, food accumulation in the esophagus, or other difficulties, contact your attending physician immediately.
Diet recommendation after implantation of the esophageal stent
The stent expands gently and keeps the narrowed area of the esophagus open, making it easier to swallow food and drinks. The stent is not as wide or flexible as a normal esophagus, so you have to be careful about some types of food and how you eat to prevent its blocking.
The most common reason for stent blockage is food that is swallowed without being sufficiently chewed, or food that does not disintegrate sufficiently when chewed. Therefore, it is recommended (for the entire time the stent is placed) to chew all bites well, or otherwise blend and drink after each mouthful.
Recommended dietary guidelines (this applies above all to esophageal stents)
- Chew the food thoroughly.
- If possible, eat 5 to 6 smaller meals a day.
- Eat slowly.
- Sit up straight when eating.
- Drink plenty of fluids between meals.
- Stay in upright position at least 30 to 60 minutes after eating.
- Food should always be prepared so that it is supple, soft and easy to swallow.
- If you ever feel a “stuck” food in your throat, drink it with a little of sparkling water.
- If you have difficulty with maintaining the weight, it is advisable to use food supplements or homemade milkshakes.
If the stent is placed through the lower esophageal sphincter (cardia), do not lie down immediately after eating, prefer rather a sitting position.
Patient's Card / Implant Card
Here you can find the current leaflet with basic information for a patient with an implanted stent. For more detailed information, contact the doctor listed on your patient card who provided the implantation, or your attending physician.
| Product | Document type | Product | Document type |
|---|---|---|---|
| BD stent | Implant Card | Boubella | Patient’s card |
| Danis stent | Patient’s card | Boubella-E | Patient’s card |
| HV Stent Plus | Patient’s card | Nitinella Plus | Patient’s card |
| Flexella Plus PULL | Patient’s card | Nitinella Plus – B | Patient’s card |
| Danis Seal | Patient’s card | Enterella Pyloroduodenal | Patient’s card |
| ELLA-BD Stent Biliary THP | Implant Card | Enterella Colorectal | Patient’s card |
INSTRUCTIONS FOR USE
| Název produktu | Typ souboru |
|---|---|
| ELLA-BD Stent Biliární THP | Instructions for use |
| BD Stent | Instructions for use |
for professionals
Here you can find the current summary of publications about ELLA products.
We also provide individual consultations and product trainings. For more information, contact us via the contact form.
BD Stent
Dilation or biodegradable stent placement for recurrent benign esophageal strictures: a randomized controlled trial
Daisy Walter, Maarten W. Van Den Berg, Meike M. Hirdes, Frank P. Vleggaar, Alessandro Repici, Pierre H. Deprez, Laurence Lovat, Bartolomé L. Viedma, Bas L. Weusten, Raf Bisschops, Renan Haidry, Elisa Ferrara, Keith J. Sanborn, Erin E. O’Leary, Jeanin E. Van Hooft, Peter D. Siersema
Endoscopy. 2018 Mar. Georg Thieme Verlag KG Stuttgart. New York, ISSN 0013-726X
At 3 months, the biodegradable stent group (n = 32) underwent significantly fewer endoscopic dilations for recurrent stricture compared with the dilation group (n = 34; P < 0.001). By 6 months, the groups were similar. The number of patients experiencing adverse events was similar between the groups.Through 12 months, the groups were similar for the EQ-5D composite score (P = 0.57). However, patients in the biodegradable stent group reported a significantly better quality of life through 12 months than patients in the dilation group based on the EQ-5D VAS (P = 0.01). Within the biodegradable stent group, the WHO performance score significantly improved compared with baseline; however, no difference was seen in the dilation group. Through 12 months, the biodegradable stent group showed a significantly higher level of activity as measured by the WHO performance score compared with the dilation group.
The use of reabsorbable ELLA stent in the treatment of benign stenosis
D. Esposito, F. Calabrese, L. Fanti, E. Viale, P. A. Testoni
Abstracts of the 24th National Congress of Digestive Diseases / Digestive and Liver Disease 50/S2 (2018) e63–e238
A total of 20 reabsorbable stents were inserted to 9 patients, one was lost on follow-up, 6 patients had a clinical and endoscopic resolution at the end of follow-up (75%), 1 had a neoplastic relapse and 1 underwent the positioning of a SEMS. The most common adverse event encountered was the formation of granulation tissue creating a substenosis in 2 (10%) patients (successfully treated with another Ella stent insertion). Self limiting bleeding was seen in 1 (5%) patient and 1 (5%) patient complained with pain controlled by mean of analgesics. The insertion of a reabsorbable stent is a safe procedure, with a success rate of 75% but with a multiple number of devices/patient needed since the use of a single stent is seldom sufficient. Such a procedure should be considered as a therapy to be used in repeated sessions similarly to dilation therapy.
Endoscopically placed stents: a useful alternative for the management of refractory benign cervical esophageal stenosis
Nogales Óscar, Clemente Ana, Caballero-Marcos Aránzazu, García-Lledó Javier, Pérez-Carazo Leticia, Merino Beatriz, López-Ibáñez María, Pérez Valderas María Dolores, Bañares Rafael, González-Asanza Cecilia.
Rev Esp Enferm Dig 2017. doi: 10.17235/reed.2017.4795/2016.
A total of 23 stents (13 FCSEMS and 10 BDS) were placed in 12 patients (median 1.92, range 1-4, 6 patients received at least one BD Stent). The technical success rate was 96% (22/23 stents). Eight patients (66.6%) maintained adequate oral intake at theendof follow-up (median 33.3 months, range 3-84 months). All patients complained of minor cervical pain after placement that was well controlled with mild analgesia. Migration was recorded in 7/23 stents (30.4%) and epithelial hyperplasia in4/23 stents (17.4%). Interestingly, migration was observed in 7/13 FCSEMS (53.8%) but not in BDS (0%; p = 0.005) cases. All the migrated FCSEMS were successfully repositioned using endoscopy. In addition, significant epithelial hyperplasia was recorded in four of 23 stent cases (17.4%), all of which involved BDS. No severe adverse events were noted.
Efficacy and tolerability of biodegradable stents for recurrent benign oesophageal strictures: The Leeds experience
N. Rabb, H. Procter, N. Burr, V. Appleby, S. Everett
25th UEG Week 2017; Oct. 28-Nov.1 – Barcelona; Spain
20 patients with 37stents were included. 30 day adverse events included 4 (11%) stent migrations and 12 (32%) with significant pain, 3 patients requiring in-patient pain control (<3 days). There were no significant bleeds or perforations.12 months following first EBS insertion 18(90%) required further endoscopic intervention due to recurrent symptoms. There was a significant reduction in median number of interventions in the 12m following EBS insertion compared to the preceding 12m (2 vs. 7 respectively, p=0.0003). Repeated EBS insertion appears a reasonable strategy for the most resistant strictures.
Single and sequential biodegradable stent placement for refractory benign esophageal strictures: a prospective follow-up study
M. M. C. Hirdes, P. D. Siersema, P. G. A. van Boeckel, F. P. Vleggaar
Endoscopy. 2012 Jul;44(7):649-54.
In total, 59 stents were placed in 28 patients. All patients had previously been treated with at least 10 dilations within 6 months; eight patients (29 %) had also been treated previously with placement of one or more SEPS or SEMS. After initial stent placement, the median dysphagia-free period was 90 days (range 14–618 days). Clinical success (absence of dysphagia ≥6 months after stent placement) was achieved in seven patients (25 %) and major complications occurred in eight patients (29 %). Three patients are currently dysphagia-free. After placement of a second biodegradable stent, the median dysphagia-free period was 55 days (range 25–700 days) and clinical success was achieved in 15% of patients. Three patients are currently dysphagia-free. After placement of a third stent, the median dysphagia-free period was 106 days (range 90–150 days), but none of the patients was clinically dysphagia-free. A possible explanation for the high complication rate may lie in the large diameter of the biodegradable stent. In seven of eight patients with major complications a 25-mm-diameter stent with 31-mm flares was placed. Conclusion: Placement of a single biodegradable stent is only temporarily effective in the vast majority of patients with RBES treated in a tertiary referral center. Sequential stenting may however be an option to avoid serial dilations.
The role of biodegradable stents in the management of benign and malignant oesophageal strictures: A cohort study
Stephen McCain, Scott McCain, Barry Quinn, Ronan Gray, Joan Morton, Paul Rice
The Surgeon (2015), http://dx.doi.org/10.1016/j.surge.2015.01.002ge.2015.01.002
17 stents were inserted to 9 patients for benign disease. Of the 9 patients who underwent a total 18 attempts at BD stenting for benign strictures, 5 were symptom free at follow-up. 4 patients with benign disease required re-intervention with a BD stent. 1 patient had 5 BD stents inserted at different time points, 1 patient had 3 BD stents inserted and 2 patients had 2 stents inserted. Median re-intervention time was 260 days (range 91-525). This study has shown BD stenting to be a very efficacious method of symptomatic relief of oesophageal stricture induced dysphagia, resulting in a significant improvement in dysphagia score post-stenting. BD stenting has an excellent safety profile, with no major complications and no stent related mortality. It would appear to offer patients with benign disease greater than 50% possibility of long-term symptom resolution. For those who require re-intervention, the duration of absence of symptoms and re-intervention time is significantly longer than would be expected with either dilatation or SEMS or SEPS.
HV Stent Plus
ELLA-HV anti-migration stent demonstrates superior performance for cancers of the gastrooesophageal junction
Mercer J, Najran P, Edwards DW, Borg P, Mullan D, Bell J, Laasch H-U
BSIR Annual meeting, Birmingham, 1st to 3rd Nov 2017
79 stent procedures were identified. There was 100% success in placing the stent across the GOJ and no reports of failure at 24 hours. Median follow up was 75 days (7-452). 4/79 (5.1%) stents migrated distally (95% CI: 1.6-12.7%), compared with 109/615 (17.7%) stent in ROST 2 registry (95% CI: 14.7-20.7%). Reduced distal migration was observed (5% significance level, p = 0.004), with a corresponding reduction in migration rate of 71.4%. The Ella HV stent confers a statistically significant reduction in distal migration compared with stent types recorded in the national registry, reducing the need for re-intervention with associated risks and cost.
A comparison of oesophageal self-expanding metal stents and their complications
C. Davidson, C. Rutherford, J. Allan, G. Simpson, J. Gray. (2016)
Royal Alexandra Hospital, GGC NHS Trust, Glasgow, UK. International Journal of Surgery. 36. S88. 10.1016/j.ijsu.2016.08.294.
A total of 98 SEMS were inserted, of which the most common were XS Ella and Niti S, with 54 and 22 inserted respectively. The remaining stent types were either not documented (19), metal (1), Ultra flex (1) or Boston Scientific Polyflex (1). Complications included blockage (total 6/98; XS Ella 2/54; Niti S 2/22) migration (total 15/98; XS Ella 0/54; Niti S 4/22) perforation (total 4/98; XS Ella 0/54: Niti S 2/22) and pain (total 7/98: XS Ella 2/54; Niti S 2/22).
Fully covered stents versus partially covered stents for palliative treatment of esophageal cancer: Is there a difference?
J.O. Alonso Lárraga, D.Y. Flores Carmona, A. Hernández Guerrero, M.E. Ramírez Solís, J.G. de la Mora Levy y J.C. Sánchez del Monte
Departamento de Endoscopia Gastrointestinal, Instituto Nacional de Cancerología, Ciudad de México, México Recibido el 30 de septiembre de 2016; aceptado el 5 de julio de 2017
A retrospective study was conducted on patients with inoperable esophageal cancer treated with self-expandable metallic stents. The 2 groups formed were: group A, which consisted of patients with a fully covered self-expandable stent (SX-ELLA®), and group B, which was made up of patients with a partially covered self-expandable stent (Ultraflex®). Group A – Technical success was achieved in 100% (n = 21) of the cases and clinical success in 90.4% (n = 19). Group B – Technical success was achieved in 100% (n = 29) of the cases and clinical success in 89.6% (n = 26). Complications were similar in both groups (33.3 vs. 51.7%) and included beside others early migration (3/21 vs. 3/26), late migration (1/21 vs. 2/26), obstruction by tumour (0/21 vs. 5/26).
Insertion of Removable Self-Expanding Metal Stents as a Treatment for Postoperative Leaks and Perforations of the Esophagus and Stomach
Inbar R, Santo E, Subch AE et al.
Israel Medical Association Journal; 2011; 13: 230–233.
Between June 2009 and February 2010 the SX-ELLA esophageal stent was inserted in five patients. The indications for stent insertion were postoperative leak in four patients and postoperative esophagopleural fistula in one patient. Three of the patients had a leak at the gastroesophageal junction following laparoscopic sleeve gastrectomy. There were no documented complaints in any of the patients regarding dysphagia or chest pain. Stents were removed electively after 6 to 7 weeks.
Safety and efficacy of self-expanding removable metal esophageal stents during neoadjuvant chemotherapy for resectable esophageal cancer
Pellen M. G. C., Sabri S., Razack A. et al.
Diseases of Esophagus; 2012; 25, 48–53.
Sixteen patients underwent esophageal stenting during neoadjuvant therapy. Tumors were located in the lower one third of the esophagus. Stent migration was anticipated in response to tumor regression. Patients were counseled that this was a potential outcome and slippages were readily retrieved endoscopically or at operation. Stents migrated during neoadjuvant therapy in 7/16 (43.8%) patients. Outcomes in our series suggest that SERMS could be considered a safe and feasible alternative methodof maintaining nutritional supplementation during neoadjuvant chemotherapy for stenosing esophageal cancers.
Danis Stent
Esophageal Balloon Tamponade Versus Esophageal Stent in Controlling Acute Refractory Variceal Bleeding: A Multicenter Randomized, Controlled Trial
Escorsell, Àngels, et al.
Hepatology, 2016 Jun;63(6):1957-67. doi: 10.1002/hep.28360. Epub 2016 Jan 14
28 patients were included – Esophageal Stent (n = 13), Balloon Tamponade (n = 15). Esophageal metal stents are more effective than balloon tamponade for the temporary control of massive or refractory esophageal AVB in patients with cirrhosis. The results of our multicenter randomized, controlled trial (RCT) show that the use of self-expandable esophageal stents provides a better balance of benefits and harms than balloon tamponade.
SX-Ella Stent Danis Effectively Controls Refractory Variceal Bleed in Patients with Acute-on-Chronic Liver Failure
Maiwall, R., Jamwal, K.D., Bhardwaj, A. et al.
Dig Dis Sci 63, 493–501 (2018). https://doi.org/10.1007/s10620-017-4686-8.
Acute-on-chronic liver failure patients (n = 88, mean age 47.3 ± 10.9 years) with refractory variceal bleeds received either Danis stent (Gr. A, n = 35) or continued with repeat endotherapy and vasoactive drug (Gr.B, n = 53). Control of initial bleeding was significantly more in the Danis stent group as compared to controls in both pre-match (89 vs. 37%; p < 0.001) and PRS-matched cohorts (73 vs. 32%; 0.007). Further, bleed-related death was also significantly lower in Danis groupas compared to controls in both pre-match (14 vs. 64%; p = 0.001) and PRS-matched cohorts (6 vs. 56%; p = 0.001). In a multivariate competing risk Cox model, patients who underwent DE stenting had reduced mortality in both pre-match (p = 0.04, HR 0.36, 95% CI 0.13–0.96) and PRS-matched cohorts (p < 0.001, HR 0.21, 95% CI 0.08–0.51). These findings highlight that Danis stent could be considered as the first-line management option for patients with ACLF with refractory variceal bleeds wherein TIPS is contraindicated.
A self-expanding metal stent for complicated variceal hemorrhage: experience at a single center
Wright G, Lewis H, Hogan B et al.
Gastrointest Endosc. 2010 Jan;71(1):71-8.
10 patients with variceal hemorrhage with contraindications to TIPS insertion or BT were followed. Stent insertion was successful in 9 of 10 patients. Insertion of the SX-Ella DANIS stent in patients with refractory variceal bleeding or complications of previous therapy is effective for the control of bleeding. In selected patients, SX-Ella DANIS stent insertion offers an alternative to other methods of salvage such as BT and TIPS and could be considered a substitute for BT after a prospective trial.
Treatment of Esophageal Variceal Hemorrhage with Self-Expanding Metal Stents as a Rescue Maneuver in a Swiss Multicentric Cohort
Fierz FC, Kistler W, Stenz V et al.
Case Rep Gastroenterol. 2013;7:97–105.
The use of variceal stenting in 7 patients with a total of 9 bleeding episodes in three different Swiss hospitals is described. Insertion of the stent led to immediate bleeding control in 89% (8/9) of patients. In all of these 8 cases no re-bleeding was observed subsequently while the stent remained in situ. Thanks to their safety and easy handling, SEMS are an interesting alternative to balloon tamponade as a bridging intervention to definitive therapy including the pre-hospital setting.
Self-Expanding Metal Stent (SEMS): an innovative rescue therapy for refractory acute variceal bleeding
Kinesh Changela, Mel A. Ona, Sury Anand, Sushil Duddempudi
Department of Gastroenterology, The Brooklyn Hospital Center, New York, USA. 2014.
At present, 103 cases have been described in the literature. Studies have reported 97.08% technical success rates in deployment of SEMS. Most of the stents were intact for 4–14 days with no major complications reported. Stent extraction had a success rate of 100%. Successful hemostasis was achieved in 96% of cases with only 3.12% found to have rebleeding after placement of SEMS. Stent migration, which was the most common complication, was observed in 21 % of patients.